
From the 1Department of Physiotherapy, College of Health Sciences, University of Sharjah, UAE, and 2Private Practice and CBP Non-Profit, Inc. (A Spine Research Foundation), Eagle, ID, USA
Objective: To explore the effect of variable durations of stretching on neural function, pain, and algometric pressure in patients with chronic myofascial pain syndrome.
Design: Randomized controlled trial.
Patients: A total of 100 participants diagnosed with chronic myofascial pain syndrome were randomly assigned to a control group or 1 of 3 intervention groups.
Methods: The 3 experimental groups received different durations of cervical spine stretching: 15, 30 or 60 s. The control group did not stretch. Primary outcome measures included peak-to-peak somatosensory-evoked potential for dermatomes C6, C7 and C8. Secondary outcome measures included central somatosensory conduction time (N13–N20), pain intensity, and pressure-pain threshold algometric measurements. All outcome measures were assessed immediately after and 2 h after the treatment session.
Results: Post hoc analysis indicated that stretching for 60 s significantly decreased the dermatomal amplitude for C6, C7 and C8 (p < 0.001) and significantly increased the central conduction time, indicating negative effect (p < 0.001). Stretching for 30 and 60 s resulted in greater improvement in pain intensity and algometric pressure than stretching for 15 s or no stretch (control) p < 0.001.
Conclusion: Stretching cervical muscles involved in chronic myofascial pain syndrome for 30 s was optimal in achieving stretching benefits and minimizing the negative effects on the neural function of the involved nerve roots and central nervous system.
Key words: stretching; randomized controlled trial; cervical; neural function; optimal stretching duration.
Accepted Nov 30, 2020: Epub ahead of print Dec 28, 2020
J Rehabil Med 2021; 53: jrm00142
Correspondence address: Ibrahim M. Moustafa, Department of Physiotherapy, College of Health Sciences, University of Sharjah, 7 Mohamed Hassan El gamal Street, Abbas El Akaad, Nacer City, Egypt. E-mail: iabuamr@ sharjah.ac.ae
Doi: 10.2340/16501977-2781
This study measured the effect of different durations of stretching (15 s, 30 s, 60 s and no stretching) of the muscles around the neck and shoulders in 100 participants with chronic myofascial pain syndrome. The outcome measures assessed the effect on neural function. The results show that stretching for 30 s was the optimal time, for achieving stretching benefits and minimizing the negative effects on the neural function of the involved nerve roots and central nervous system. Stretching for a longer time negatively affected the neural function, but decreased the pain level, while stretching for a shorter time did not achieve the optimal muscle length after stretching.
Chronic myofascial pain syndrome (CMPS) is a syndrome of musculoskeletal pain that is typically linked to myofascial trigger points (MTrP) (1, 2). CMPS is mostly prevalent in muscles that are consistently active against gravity or muscles that are essential in repetitive activities, such as the head, neck, shoulders, hips and low back muscles (3). The postural muscles that most commonly tend to be shortened are the upper trapezius and levator scapulae, resulting in limited neck mobility (4) and, due to the continuous demand on these muscles to maintain an upright posture, there appears to be a strong justification for stretching them.
Current approaches to the management of CMPS include pharmacological and non-pharmacological interventions (5–7). Among the non-pharmacological approaches, many studies have supported stretching exercises as a beneficial intervention to treat CMPS (8–11). Overall, while the results of these studies are not specific to stretching alone, stretching exercises appear to be an important component of CMPS management. While the benefits of stretching are known, controversy remains about the stretching parameters needed to achieve a particular goal or treatment outcome. In clinical practice, multiple stretching techniques are used; nevertheless, there is no evidence-based agreement on the most effective parameters. One of the parameters that might affect treatment outcome the most is stretching duration; however, to date, there is a little agreement about the optimal duration of stretching (12–15).
Of interest, comparison and subsequent conclusions about appropriate stretching times are based mainly on mechanical factors, such as range of motion and flexibility, while ignoring the neural adverse mechanical tension that may be created during sustained stretching exercises. According to the literature (16–18), stretching induces neural tension that may adversely affect the central nervous system and nerve root function, due to the absence of the perineurium, which is the primary load-carrying structure. Thus, safe or unsafe limits of nerve elongation are not well established, despite several basic scientific and clinical studies (19). It is thought that the same phenomenon of tissue loading is applicable to the nervous system. The literature indicates that the most offensive: the most structure damaging postural loading of the central nervous system and related structures occurs in any procedure or position requiring spinal flexion (20).
Consequently, the current study aimed to determine whether increased longitudinal strain and stress on the spinal cord and nerve roots from continuous stretching exercises could subtly impair neural function. The study hypothesis is that there is a duration threshold, beyond which adverse neural function will be apparent, resulting in a reduction in either or both latency and amplitudes of evoked potentials.
A prospective, blinded, parallel-group, randomized clinical trial was conducted in the research laboratory of our university in Egypt (Physiotherapy Research Lab, Cairo University, Cairo (the university has multiple departments of physiotherapy with a common research lab). The trial was registered with ClinicalTrials.gov (NCT04190784). Recruitment began after approval was obtained from the university research ethics committee. The patients participated in the study after signing an informed consent form prior to data collection.
Inclusion criteria
Participants who had active, palpable MTrP on the upper trapezius muscle uni- or bi-laterally, and persistent neck and/or shoulder regional pain, for at least 8 weeks preceding the study were included consecutively. One examiner, with 12 years’ experience, performed a thorough musculoskeletal evaluation to diagnosis the myofascial pain and rule out other causes of muscle pain. Participants were included based on Simon’s diagnostic criteria, which required 5 major criteria to be satisfied: 1: regional pain; 2: referred pain; 3: a taut band; 4: a tender point in the taut band; and 5: restricted range of motion; and at least 1 of the 4 minor criteria: 1: pain reproduced by pressure on the tender spot; 2: snapping palpation of the taut band at the MTrP elicits a local twitch response; 3: relief of pain with injection, or by stretching; and 4: electromyographic demonstration of spontaneous electrical activity (21).
Exclusion criteria
Exclusion criteria included any signs or symptoms of medical “red flags”, such as: tumour, osteoporosis, fracture, rheumatoid arthritis, and prolonged use of steroids. Participants were also excluded if they had a history of spinal surgery and any objective findings consistent with neurological conditions and vascular disorders. Furthermore, they were excluded if they had received physical therapy, or any local trigger point injection during the 3 months prior to starting the study, which might affect the results during treatment or follow-up periods
Participants were divided into 4 groups according to the duration of stretching (15, 30 and 60 s; the fourth group, which served as a control, did not stretch). Participants were randomly assigned to one of the 4 groups as described below. The randomization process was based on permuted blocks of variable sizes. Each random permuted block, created by random a number generator, was transferred to a sequence of consecutively numbered, opaque, sealed envelopes, which were kept in a locked drawer until needed. Once a participant was formally included in the trial, the next envelope in the sequence was opened by the researcher in the presence of the participant, who would be assigned to a group according to the number in the envelope (and the participant would still be blinded to the group to which they were assigned).
Stretching for upper trapezius and levator scapula
From the supine position, the examiner passively placed the participant’s cervical spine into flexion, rotation to the ipsilateral and side-bending to the contralateral side of the stretched upper trapezius. For the levator scapulae, the cervical spine was placed in flexion, rotation, and side-bending to the contralateral side. The stretch was just short of the restriction barrier (i.e. once the muscle was taken into the restriction barrier the therapist backed off a range of motion (ROM) degrees from that position). The participant introduced a light resisted effort (20% of available strength) to bring the ipsilateral shoulder towards the ear and side-bend the head to the ipsilateral side
The contraction was held for 10 s and, once there was a complete relaxation of effort, the treating therapist gently took the cervical spine into more range of motion of side-bending and appropriate rotation; stabilization of this position was required at this point, as the shoulder was caudally stretched.
All interventions were delivered individually by the same physiotherapist, who has a PhD in physiotherapy and 15 years of clinical experience, and who received training in these manual techniques in order to minimize inter-therapist variation and enhance fidelity.
A force of 100 N, measured using a pressure dynamometer, was used by the examiner to depress the participant’s shoulder. Once the examiner achieved this level of force, he maintained the stretch for 15, 30 or 60 s (using a timer) according to the experimental group. The patient relaxed for approximately 20 s and the procedure was repeated 3 times.
Control group
The control group followed the same procedures, except that no stretching force was applied at the end. The assessor, who took the measurements for both the intervention and control groups, was blinded to the participant’s group, while the treating therapist was not blinded to the treatment intervention.
Outcome measures
Assessments of the outcome measurements were performed at 3 time-points: pretreatment, immediately after treatment and 2 h after treatment. The primary outcome measure for determining treatment assessment was dermatomal somatosensory-evoked potentials (DSSEPs).
Dermatomal somatosensory-evoked potentials
In all dermatomes, 2 complete recording runs were undertaken during each session, with averages of 250–1,200 cortical responses from scalp surface recording electrodes (C3’–C4’ in a 10–20 electrode configuration) of the contralateral scalp to the C6, C7, and C8 dermatomes being stimulated. The impedance of ground and scalp electrodes was maintained at < 5 k ohms) (22–24).
Secondary outcome measures
N13–N20 potential. A standard clinical technique for upper limb stimulation (median nerve at the wrist) was used to determine the central somatosensory conduction time measurement, N13–N20, for each participant (22–24). The central conduction time was measured from the peak latency of the N13 component in the Cv6-to-Fz montage to the peak latency of the N20 (P20 component in the Pc-to-Fz montage).
Pain intensity. The numerical pain rating scale (NPRS) was used to measure the intensity of neck pain (25).
Pressure-pain threshold algometric measurement. In order-to assess the pressure-pain threshold (PPT) at the most tender point on the upper trapezius muscle, a pressure threshold algometer was used. This measurement was repeated 3 times with 30–60-s intervals in between. The mean value of the 3 repetitions (in kg/cm2) was used in data analysis of PPT (26–27).
All outcome assessments were carried out by the same assessor, who was blinded to group allocation and had 12 years’ experience in neurophysiological and pain assessment.
Sample size determination
To determine the required number of participants needed in this study, estimates of mean and standard deviations (SD) were collected from a pilot study consisting of 10 participants who received the same programme. The mean differences and SD of the peak-to-peak amplitude of DSSEPS for different levels C6, 7, and 8 at different stretching durations: 15, 30 and 60 s, were: C6: –0.28 (SD 0.5), –0.14 (SD 0.8), –0.71 (SD 0.4); C7: –0.1 (SD 0.7), –0.4 (SD 0.6), –1.32 (SD 0.3); C8: –0.2 (SD 0.7), –0.7 (SD 0.5), –1.1 (SD 0.4), respectively. These values were used to calculate the sample size separately for each of the primary outcomes by applying a Bonferroni correction to adjust the significance level. The largest value of the sample size was then considered as the final sample size for the trial. Accordingly, at least 20 participants in each group, given a statistical power of 80%, were needed in the current study. The sample size was enlarged by 25% to account for potential dropouts.
Data analysis
Initially, and as a pre-requisite for parametric analysis, data were screened for normality by using the Kolmogorov-Smirnov and Shapiro-Wilks normality tests. In addition, the data were screened for homogeneity of variance. Once data were found not to violate the normality and homogeneity of variance assumptions, a parametric analysis was conducted.
The comparative treatment effects of the different stretching durations were examined with 2-way analysis of variance (ANOVA) with repeated measures. The models used the group as the independent factor, time as the repeated measure and the product group × time as the interaction factor. Post hoc comparisons with Bonferroni correction were implemented when interactions were found (p < 0.05). The study adopted an intention-to-treat analysis of the results. The significance level for all analyses was set at α = 0.05. SPSS version 20.0 software (SPSS Inc., Chicago, IL, USA) was used for all data analysis.
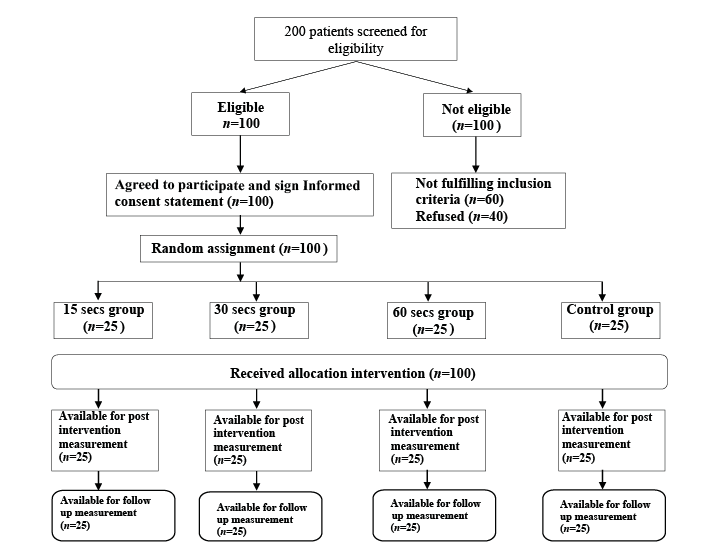
A diagram of participant retention and randomization throughout the study is shown in Fig. 1. The initial sample included 200 potential participants. Sixty participants (30% of total initial sample) did not meet the inclusion criteria or had one of the exclusion criteria, while 40 participants (20% of total sample) refused to participate. The study’s inclusion criteria were met by 100 of the initial participants approached. In total, 100 (100%) participants completed the entire study; the first measurement immediately after intervention and the second measurement after 2 h.
Fig. 1. Study flow: participant retention and randomization.
Sample characteristics
Table I presents the descriptive data for the clinical and demographic variables. These baseline variables have no statistically significant differences among the 4 groups of the study.
Table I. Baseline participant demographics of the 4 groups (G1–G4)
Neurophysiological outcomes
A 2-way repeated measures ANOVA revealed significant group × time effect on measures of pain intensity, PPT, CCT, C6, C7, and C8 p < 0.001 (Table II).The post hoc analysis indicated that stretching for 60 s significantly decreased the DSSEPs amplitude for C6, C7 and C8 (p < 0.05) and significantly increased the central conduction time (p < 0.05) (Table III) (Fig. 2).
Table II. Two-way repeated analysis of variance (ANOVA) table
Table III. Post hoc analysis matrix
Fig. 2. Neurophysiological parameters pre-, immediately post- and 2-h post-treatment for (a) dermatome C6, (b) dermatome C7, (c) dermatome C8 and (d) CCT: central conduction time measured with the N13-N20
Pain intensity and pain pressure threshold
A 2-way repeated measures ANOVA revealed significant group × time effect on measures of pain intensity, and PPT (Table II). Post hoc analysis indicated that stretching for both 30 s and 60 s significantly increased the pain pressure thresholds and decreased the pain intensity compared with the 15 s and the control groups (p < 0.05) (Table III) (Fig. 3).
Fig. 3. Pain and algometric pressure measurements pre-, immediately post- and 2-h post-treatment.(a) Algometric pressure and (b) pain measurements pre-, immediately post- and 2-h post-treatment
The differences between groups indicate that different stretching durations had an effect on central conduction time, DSSEPs and other management outcomes. Thus, the primary hypothesis of the current study is confirmed by these findings. Stretching the upper trapezius and levator scapula muscles for 30 s and 60 s resulted in greater improvements in pain intensity and algometric pressure than stretching for 15 s or no stretch (control). However, regarding the neurophysiological parameters, stretching the upper trapezius and levator scapula muscles for 60 s adversely affects the peak-to-peak amplitudes of C6, 7 and 8. Furthermore, stretching for 60 s adversely affected central conduction time and these negative impacts lasted for at least 2 h. Since 60 s of stretching did not result in any additional benefits compared with 30 s of stretching regarding pain and algometric pressure, the use of longer stretches should be avoided.
Based on these results, stretching for 15 s or 30 s was safer with respect to the neural function measured with evoked potentials. Considering the minimal change in pain intensity and algometric pressure after 15 s, the results of this study suggest that the most effective duration of stretching is 30 s. To our knowledge, this study is the first of its kind to present objective evidence that relates different stretching times to these specific neurophysiological parameters.
Stretching studies vary by the different muscles or muscle groups that are being examined and the variety of populations studied, thereby making interpretation and recommendations somewhat difficult. The current study cannot be directly compared with the results of others, due to the differences in methodology and the cervical specific stretches that were tested. Still, the novel result of the current study is that 60 s stretching significantly decreases the peak-to-peak amplitude of the DSSEPs tested, in addition to increasing the central conduction time. One of the primary mechanical mechanisms that could lead to neurological dysfunction is the increased longitudinal tension in the nerve root and spinal cord tissues. Furthermore, spinal cord and peripheral nervous system biomechanics might explain our finding of increased central conduction time and decreased amplitude of DSSEPS after 60 s of stretching (20, 28). It has been found that neural axoplasm has thixotropic properties, which indicates that lack of motion or increased sustained strain will increase the viscosity of fluid flow and may slow or impair neural transport mechanisms (29).
Furthermore, to maintain an optimal structure and function the neural tissue needs abundant amounts of oxygen and multiple other nutrients. The neural tissue has high energy expenses, even when the homeostatic environment is stable. This energy is crucial for the operation of cellular mechanisms, such as biosynthesis, axoplasmic transport, neurotransmitters metabolism and operation of the ionic pumps (30). It has been proven that continuous stress on the spinal cord will directly affect blood flow to the meningeal complex and may decelerate or impair the neural transport processes (31, 32). The biomechanics of the nervous system may explain the significant decrease in the amplitude after 60 s of flexion stretching in the current study. This idea of relating the dynamic forces applied on the neural tissue to the impairment seen in the neural function is in agreement with the concept described by Brieg (33), who proposed that the cross-sectional area of the spinal cord decreases with spinal flexion, while the spinal cord and nerve roots fold and relax in extension. Consequently, the neural tissue will be exposed to a harmful mechanical stress, in which the nerve root sleeves unfold and become strained, and the blood supply is decreased with a reduced lumen cross-sectional area (34, 20).
Several studies provide support for the above concept. One study reported that neurogenic motor-evoked potentials and somatosensory-evoked potentials after spinal cord distraction detected a meaningful decrease in afferent and efferent impulse conduction (32). Other case studies reported that sustained postural deformities, such as spinal scoliosis, may cause similar neuronal function impairments to these that occur with distraction instrumentation used on the spine, spinal cord, or those that happen in tethered cord syndrome (33).
Pain
Stretching for either 30 or 60 s seems to be similarly effective in decreasing the pain intensity and increasing the PPT. The acute effect of Muscle Energy Technique (MET) is consistent with the findings of many authors, who reported an immediate reduction in pain associated with trigger points after applying a MET technique (35, 36). Decreased pain could be attributed to acute ischaemic compression after the stretching phase, which has been shown to result in reduced perceived pain in the neck and shoulder muscles (37); this may be why longer stretching times have more impact on pain reduction.
Study limitations
This study has several limitations, indicating the need for further research. First, the short-term follow-up of 2 h after the intervention was terminated. Secondly, the current study was limited to lower cervical nerve roots, which were selected because they are the most vulnerable nerves that may be affected during flexion stretching positions. In addition, the current study was limited to the immediate effects of a single session of stretching. Future research is needed to evaluate the effects of treatment programmes using typical frequency and duration of care for CMPS and to determine the long-term effects, if any.
This study showed that stretching the cervical muscles involved in CMPS for 30 s was optimal in achieving stretching benefits and minimizing the negative effects on the neural function of the involved nerve roots and central nervous system. A longer duration of stretching had a negative effect on the neurophysiology variables of the nerves involved in the muscles stretched. These results should assist in optimizing the stretching time of involved tissues in order to achieve the well-established goals from stretching, while avoiding any negative effects on neural function.
The author have no conclicts of interest to declare.


 Click to show fullsize
Click to show fullsize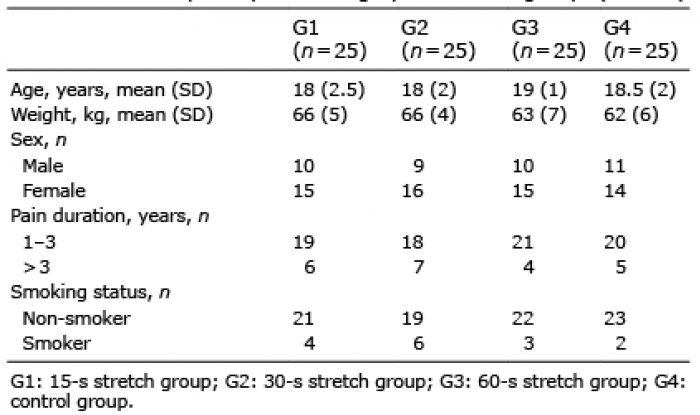 Click to show fullsize
Click to show fullsize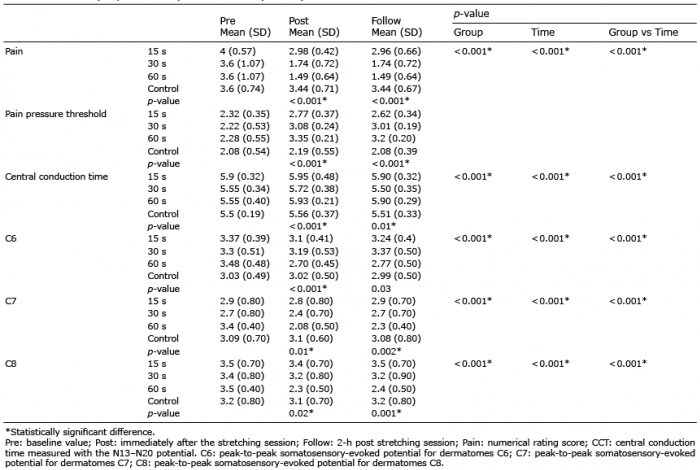 Click to show fullsize
Click to show fullsize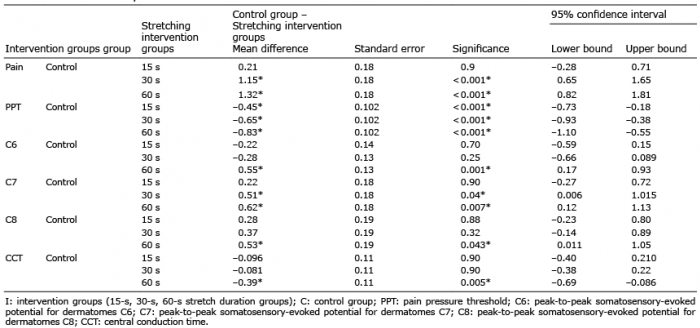 Click to show fullsize
Click to show fullsize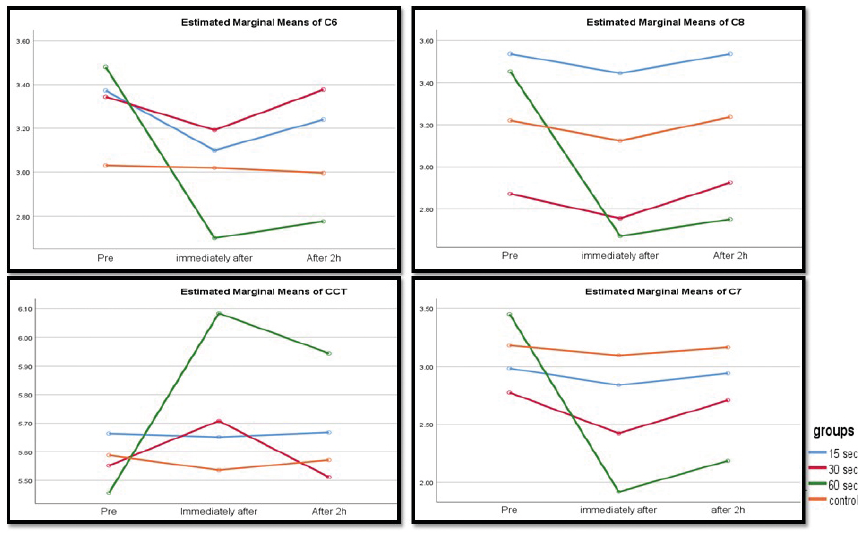 Click to show fullsize
Click to show fullsize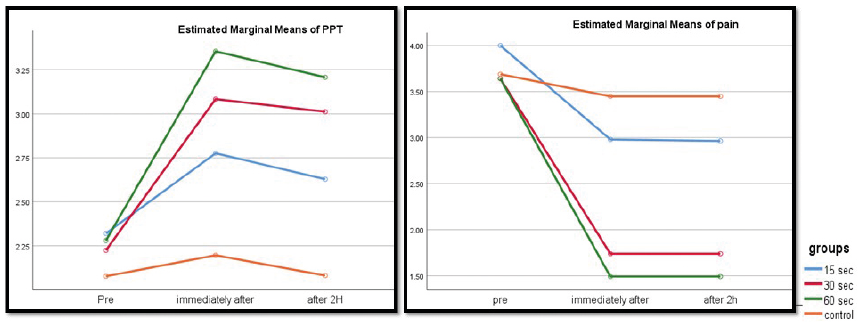 Click to show fullsize
Click to show fullsize